
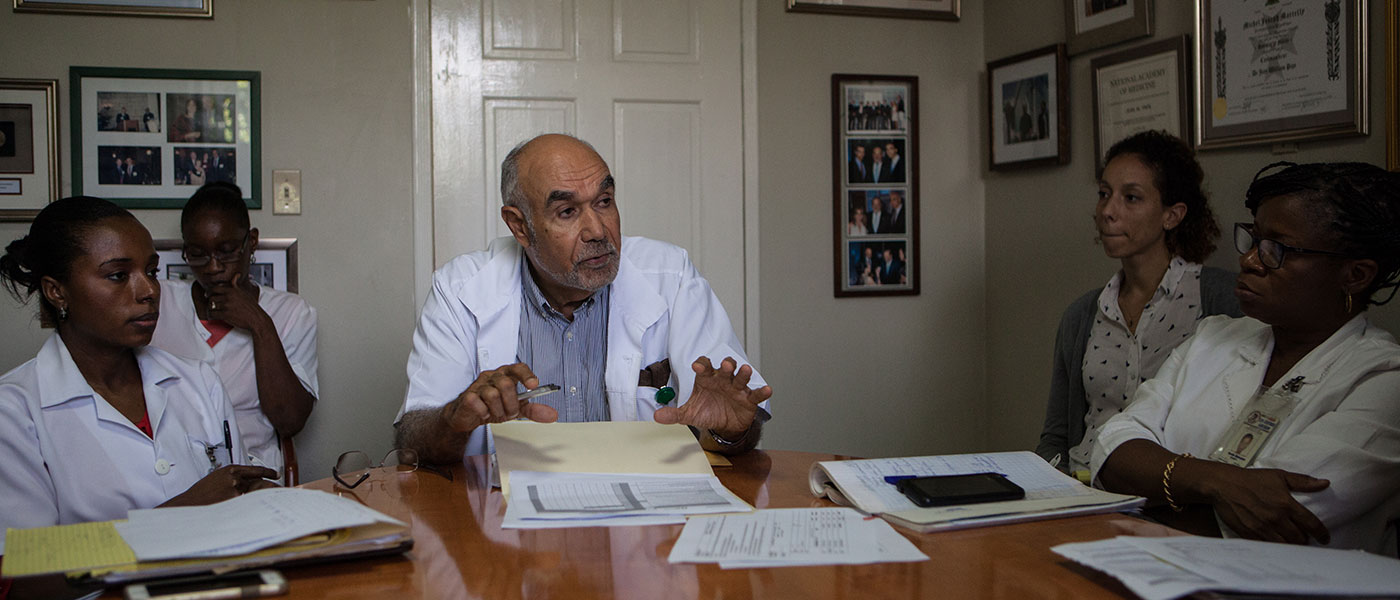
Dr Jean William “Bill” Pape was born in Port-au-Prince, Haiti. He studied medicine in the United States and specialized in internal medicine and infectious diseases. Currently, he is Professor of Clinical Medicine at the Center of Global Health at Weill Cornell in the USA and Director of Centres at GHESKIO in Haiti. The focus at GHESKIO is treatment of HIV and tuberculosis. Jean Pape has experienced some of Haiti’s most difficult events, including the 2010 earthquake …
The earthquake in 2010 was the biggest challenge we have ever faced. We had many difficult things happen through the ’90s and ’00s, but the earthquake was the worst. I was not sure whether we would overcome it because, in addition to taking care of people that presented with infectious and chronic diseases, we had to treat others with unimaginable injuries.
The earthquake killed over 250,000 people, displaced 1.5 million others, and was estimated to have caused between US$7.8 billion and US$8.5 billion in damage. It destroyed public buildings, including all the hospitals, which prevented many clients from accessing life-saving medical care and treatment, including for tuberculosis (TB), for weeks. The earthquake also affected our staff a lot. We lost four people, including the head of the microbiology lab. About 60% of our staff lost one or more person in their family and 70% had their house either destroyed or severely damaged.
The impact of the earthquake in communities was huge because 1.5 million people were internally displaced. They occupied all available public spaces (soccer fields, parks…) and were living in tents.
“We had families, mothers and infants in the tents, and some of them were sick with TB.”
In those tents with limited or no ventilation, we were concerned about a higher risk of TB transmission. And then, the very same year, we had a cholera epidemic. We were not done dealing with the devastation brought by the earthquake when the severe cholera outbreak happened. So we had two catastrophes at the same time. In addition, we knew that we were going to have another public health problem when we started to see more pediatric cases of TB. Indeed, in 2010, we had four times the number of TB cases among children than in 2009. Children being sentinel cases, we knew we were going to have a huge increase in TB patients.

The first thing we had to do after our TB hospital collapsed was to put each person that was living with drug-resistant tuberculosis (DR-TB) into a separate tent so that we could provide them with adequate care. The second thing we did was to establish a functioning medical laboratory. When we received people presenting with TB symptoms and signs, we managed to diagnose TB and placed them on treatment the same day, which helped to cut the chain of transmission. If we had let any of them go without treatment it would mean to them that their medical condition was not serious enough as it did not require immediate care. For sure, they would not have come back.
“In my opinion, it is extremely important to always diagnose and start TB treatment on the same day a TB diagnosis is made.”
Presently there are 169 centres in Haiti providing TB treatment and antiretroviral care for HIV nationwide. It is also essential to evaluate all TB clients for HIV, and all clients living with HIV for TB, since HIV and TB often occur at the same time in the same person.
In a project we conducted with the support of TB Reach, we found that up to 20% of adults with chronic cough in a heavily populated poor urban area in Port-au-Prince had active TB and the rate of HIV was four times higher in this group than in the general population. Staff should therefore be extremely attentive to clients coming for HIV testing and presenting with a cough. It is a great opportunity to diagnose and treat active TB as well as prevent active TB. Most of the people seeking an HIV test who turn out to have TB will be HIV-negative. Those who are HIV positive and do not have active TB can be placed on TB prophylaxis. We have had a great experience with early isoniazid treatment in preventing active TB among people living with HIV. In the region, Haiti is now the country with one of the highest rates of isoniazid use as prophylaxis in people living with HIV.

“Despite great progress, DR-TB continues to be a challenge.”
We have set up a supportive DR-TB programme with our clients. Once their sputum culture is negative, clients are actively followed with directly observed treatment at home during the remaining two years of the treatment course. We are reaching success rates of 80% with a 7% loss-to-follow-up and 9% mortality rate. We are currently piloting a new short 39-week course for MDR-TB and seeing very encouraging preliminary results.
“Stigma is the last challenge we face when working with TB and HIV in Haiti.”
We have a strong community advisory group with a variety of members, including people living with HIV. They have helped us decrease the stigma related to HIV and TB. However, this is a constant effort and challenge that continues to perpetuate vulnerability to HIV and create barriers to accessing services for some communities as there are religious and political leaders who continue to stigmatize men who have sex with men. We have conducted specific training for our staff to make sure that we welcome everyone regardless of their sexual orientation. We have also used a mobile clinic truck that stops at hot spots where men who have sex with men and female sex workers gather. We employ people from these groups to help us reach different populations in order to offer them HIV and TB services.
All these methods have worked for us. Challenges persist, but we have made constant progress against all odds. HIV and AIDS used to be the number one killer in Haiti for two decades but is now the seventh cause of mortality in Haiti accounting for 5.7% of all deaths. We remain focused to combat HIV and TB and determined to deliver the best quality care for HIV and TB in Haiti.